Introduction
Since its passage in 1965, Medicaid has provided vital health insurance coverage to some of the most vulnerable populations in America. In order to remain solvent, Medicaid relies on its program administrators and contractors to be fiscally responsible. For that reason, third party liability (TPL) is critically important, not just for Medicaid, but for all its beneficiaries and any policymaker who cares about the healthcare safety net. However, the identification of TPL has been problematic and is costing Medicaid billions of dollars annually.
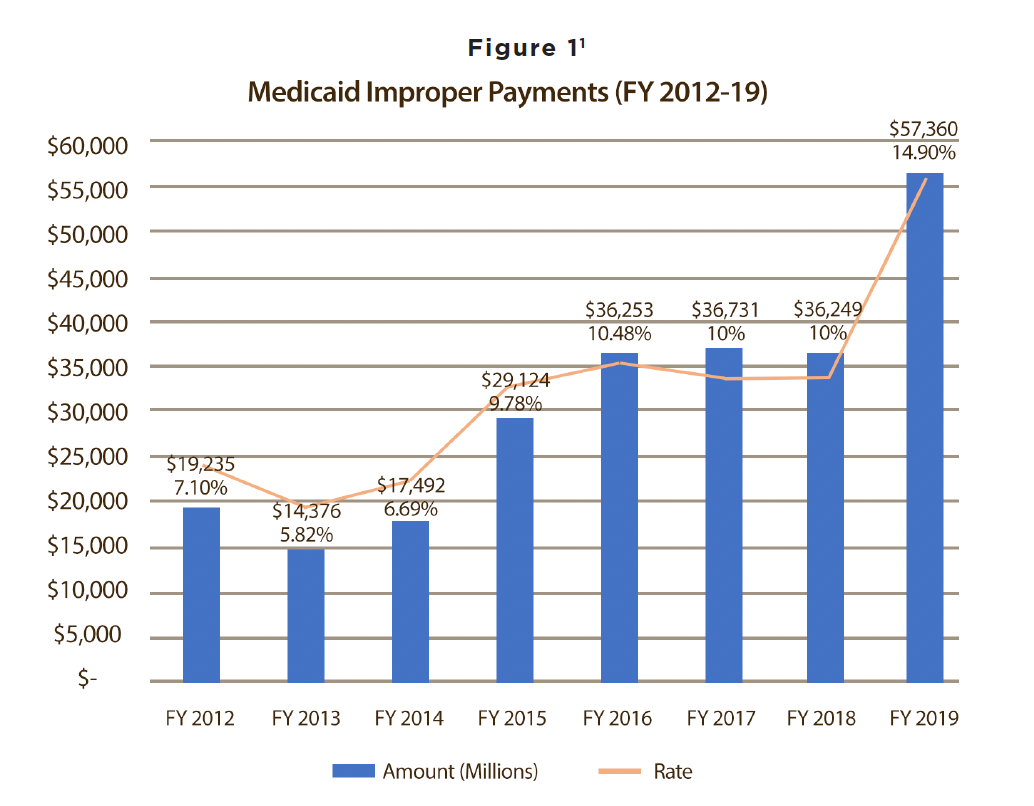
States have always been required by law to seek out third parties that may actually be liable for Medicaid beneficiaries’ claims. However, ‘seeking’ is simpler in concept than in practice. For over 50 years, Medicaid administrators have struggled with TPL, one reason being that for the past 40 years, the technology needed to accurately identify TPL and cost-avoid has not existed. Federal initiatives to rein in costs have occurred, though. Numerous laws have been passed, regulations have been formulated, hearings have been held, and Government Accountability Office (GAO) and Office of the Inspector General (OIG) reports have been written and given to Congress. All have been aimed at improving the TPL process, thereby reducing Medicaid liabilities; nonetheless, states struggle with prompt, accurate determinations of TPL. Despite legislative efforts and existing TPL processes, Medicaid improper payments have risen to a rate of 14.90%, representing over $57.36 billion on an annual basis.
Saying that states must seek out TPL is only the tip of the iceberg. According to 42 CFR 433, Subpart D, “States are responsible for having plans in place to identify Medicaid beneficiaries’ other sources of health coverage, determine the extent of the liability of such third parties, avoid payment of thirdparty claims, and recover reimbursement from third parties after Medicaid payment if the state can reasonably expect to recover more than it spends in seeking reimbursement.” 2 Each step in this process can be difficult because identification of other sources of coverage for the purposes of costavoidance is particularly problematic.
Cost avoidance is far more preferable to the conventional practice of recouping improper claims payments, also known as “pay and chase.” ‘Pay and chase’ occurs when 1) payments are made in good faith by a payer of last resort, 2) that payer discovers the payments were made in error and were in fact the responsibility of another third party payer, 3) the payer of last resort seeks to rectify this by trying to recoup funds from the responsible third party payer. This is time-consuming, costly, and often fruitless. As one might imagine, third parties do not want to pay, as they are looking out for their own bottom lines, just as Medicaid programs are working to be good stewards of their resources.
Why Pay and Chase Has Been Normalized
 The ability to identify liable third party payers before claims are paid improperly has been a chronic challenge due to:
The ability to identify liable third party payers before claims are paid improperly has been a chronic challenge due to:
- Antiquated technology
- Siloed data systems
- Network latency
Medicaid plans because of unreliable eligibility data – often pay claims that were not, in fact, their responsibility. When new eligibility information or new data are made available, and plans discover overpayments, the “chase” begins.
The practice of ‘pay and chase’ has become normalized, even though cost avoidance and routing claims to the proper payers is the only way to ensure federal dollars are not paid in error. Furthermore, an entire multi-billion-dollar industry has been built around the business of post-payment recovery. Unfortunately for payers trying to recoup improper claims payments, the actual funds recovered remain around twenty cents on the dollar.
On another, practical front, it is understandable that plans may sometimes pay so as not to drag out the claims payment process. When coordinating benefits causes claims payments to be delayed, providers become dissatisfied, and this could result in providers choosing not to participate in Medicaid. There is already a shortage of providers willing to accept Medicaid, so rather than exacerbate this problem; Medicaid plans pay, even if it means they will have to chase those dollars later.
Early Legislative Efforts to Combat Improper Payments
Employee Retirement Income Security Act of 1974 (ERISA)
After the passage of Medicaid in 1965, the program evolved with the enactment of subsequent legislation. Notably, Congress passed the Employee Retirement Income Security Act of 1974, now commonly known as ERISA. This law was aimed at self-insured companies and made sure that they abided by the same health insurance requirements as other large group plans. A byproduct of this main goal was making self-insured plans subject to Medicaid TPL stipulations.
Improper Payments Information Act (IPIA) 2002
Decades later, Congress passed the Improper Payments Information Act (IPIA) in late November of 2002. According to the Congressional Research Service, this law “requires agencies to identify each year programs and activities vulnerable to significant improper payments, to estimate the amount of overpayments or underpayments, and to report to Congress on steps being taken to reduce such payments.” To comply with this new Act, the Payment Error Rate Measurement (PERM) was developed. PERM reviews Medicaid and CHIP data to measure improper payments and estimate program-level error rates.
Deficit Reduction Act of 2005 (DRA)
A mere three years later, Congress passed the Deficit Reduction Act (DRA) of 2005. It added more entities to the list of those considered third parties. All entities defined as third parties are required by law to comply with Medicaid TPL processes, including the supplying of beneficiary eligibility information to states (much like ERISA dictates for self-insured plans). The DRA also added requirements intended to enhance cooperation in data sharing between third parties and states. Another part of the DRA was the Medicaid Integrity Program. This allowed contractors to review Medicaid provider activities, audit claims, identify overpayments, and educate providers and others on Medicaid integrity issues.
2006 GAO Report – Medicaid
Third Party Liability: Federal Guidance Needed to Help States Address Continuing Problems
By September 2006, the GAO concluded that further federal guidance was necessary to curb improper Medicaid payments. They found that about 13% of Medicaid beneficiaries had some other health coverage during any given year. Based on this statistic, more than 1 in 10 Medicaid beneficiaries may be having claims covered by Medicaid that in fact should be paid by a third party. This 2006 GAO report also found that while the DRA moved the ball forward on TPL, there were some technical discrepancies necessitating more detailed federal regulation. In other words, while states were trying to comply with DRA provisions, their efforts were hampered by a lack of clarity.
Post Deficit Reduction Act
Qualifying Individual Program Supplemental Funding Act of 2008 (QI)
Although the Public Assistance Reporting Information System (PARIS) was first initiated in 1993, the Qualifying Individual (QI) Program Supplemental Funding Act of 2008 changed state participation requirements. It required states to link their eligibility systems through PARIS, providing data for matching purposes across participating entities. CMS found that beneficiaries crossing state lines were one source of improper payments because a mechanism did not exist for states to share information and match beneficiary information.
2009 Executive Order 13520 – Reducing Improper Payments and Eliminating Waste in Federal Programs
A few years later, in 2009, President Barack Obama signed Executive Order 13520, another effort to reduce Medicaid improper payments. It aimed to intensify efforts to eliminate payment errors, waste, fraud, and abuse while still ensuring that Medicaid and other federal programs would continue to serve their beneficiaries. Two of these intensified efforts included identifying federal programs with the highest dollar amount of improper payments and establishing reduction and recovery target rates.
Improper Payments Elimination and Recovery Act of 2010 (IPERA)
Following EO 13520, Congress passed the Improper Payments Elimination and Recovery Act of 2010. It took several steps to further increase data sharing, coordination between state agencies and third parties, and increase reporting requirements. These included but were not limited to:
Amendment of the 2002 Improper Payments Information Act (IPIA) to require the leader of each federal agency (in the case of Medicaid, the Secretary of HHS) to review and identify susceptibilities in their programs that could lead to improper payments
Revisions of the requirements related to improper payment estimations
Requirement of a statement from agencies as to whether it has “sufficient resources with respect to internal controls, human capital, and information systems and other infrastructure to prevent improper payment”
2013 HHS-OIG Report – Medicaid Third Party Savings Increased, But Challenges Remain
HHS OIG data has shown that in cost avoidance efforts, states are most successful in working with Medicare, which represents the largest proportion of cost avoidance savings for the Medicaid program. Conversely, in pay and chase efforts, health insurance companies represent the largest proportion among payers, suggesting they may be less willing to share information up front.
The 2013 HHS OIG report, similar to the 2006 GAO report, found that more federal guidance was needed and recommended closer cooperation between the federal government and states to address longstanding challenges and strengthen enforcement mechanisms for uncooperative third parties.
2015 GAO Report – Additional Federal Action Needed to Further Improve Third-Party Liability Efforts
These provisions were meant to significantly improve improper payment liability nationwide, and according to the GAO, states identified about $13.6 billion in combined federal-state cost savings from private health insurers in 2011 compared to about $3.7 billion in 2001, a remarkable 268% increase.
Most Recent Efforts
Fraud Reduction and Data Analytics Act of 2015
In recent years, Congress has taken several meaningful steps forward to improve TPL. In 2015, it passed the Fraud Reduction and Data Analytics Act, which required the Office of Management and Budget (OMB) to develop new guidelines for federal agencies. Under the act, agencies needed to “establish financial and administrative controls to identify and assess fraud risks,” and they were also required to submit annual reports to Congress regarding their progress on these efforts.
Federal Improper Payments Coordination Act of 2015 Medicare and CHIP Reauthorization Act of 2015 (MACRA) Most Recent Efforts
At the end of that same year, Congress passed the Federal Improper Payments Coordination Act. This authorized the judicial branch, legislative branch, and also state government agencies managing federal programs to utilize the U.S. Treasury Department’s Do Not Pay (DNP) Program. According to the Treasury, DNP is a “no-cost robust analytics tool which helps federal agencies detect and prevent improper payments made to vendors, grantees, loan recipients, and beneficiaries.” 16 Through both of these 2015 laws, Congress addressed administrative procedures, reporting requirements, and data- sharing, all designed to improve cost-avoidance and address TPL.
Medicare and CHIP Reauthorization Act of 2015 (MACRA) Most Recent Efforts
One of the most significant pieces of health policy legislation passed since the Affordable Care Act was the Medicare and CHIP Reauthorization Act of 2015 (MACRA). This lengthy law includes several sections pertinent to Medicaid programs, including a section affecting TPL issues. It instructed the Secretary of HHS to look at “incentives for states to work with the Secretary under the Medicare-Medicaid Data Match Program.” 17 With this provision, again Congress was seeking to increase data sharing. Shortly after the legislative progress made in 2015, there were developments in the Medicaid Management Information Systems (MMIS) in 2016. MMIS is a mechanized claims processing and information retrieval system that state Medicaid programs must use in order to receive their federal matching dollars. 18 Fraud Reduction and Data Analytics Act of 2015 Federal Improper Payments Coordination Act of 2015 Medicare and CHIP Reauthorization Act of 2015 (MACRA) Most Recent Efforts.
Shortly after the legislative progress made in 2015, there were developments in the Medicaid Management Information Systems (MMIS) in 2016. MMIS is a mechanized claims processing and information retrieval system that state Medicaid programs must use in order to receive their federal matching dollars.
2015 GAO Testimony to Congress – Overview of Key Issues Facing the Program
Also in 2015, the GAO yet again recommended more federal action to improve TPL efforts. The estimate that 13% of Medicaid beneficiaries had other coverage remained unchanged since 2006, 9 years previous. Notably, this statistic varies across age groups, with only 8.4% of children with a third-party payer and potentially up to 34.5% of the elderly population. This suggests that states were on the right track with greater cooperation with Medicare; the elderly population is where they could make great progress on TPL. However, the issue remains of how to increase cooperation from non- governmental payers. The state of Minnesota reported – via the GAO report
– impressive gains in TPL identification. It had saved about $50 million over five years by contracting with a vendor for electronic data matching. Simultaneously, CMS expanded the Recovery Audit Contractors (RAC) program. First piloted in 2005 in Medicare fee-for-service billing, this program allows outside contractors to audit provider records for purposes of identifying overpayments and underpayments. In 2016, this tactic was expanded to Medicaid TPL.
2017 GAO Report – Further Action Needed to Expedite Use of National Data for Program Oversight
After all the progress of 2015 and 2016, the GAO issued a 2017 report with alarming evidence that the Medicaid TPL problem was still not under control. The GAO states that Medicaid was responsible for one-quarter of all government-wide improper payments, totaling to nearly $36.7 billion in wasteful spending.
Data procurement and matching made another move forward again in 2018 with the advent of the Transformed Medicaid Statistical Information System (T-MSIS). This system is CMS’s attempt to bring all disparate systems together, but it is still years away from completion.
Payment Integrity Information Act of 2019 (PIIA) Most Recent Efforts (Continued)
Currently pending is S. 375, a bill that passed the U.S. Senate by unanimous consent, titled the Payment Integrity Information Act of 2019. Like previous legislation, this bill updates and strengthens federal agencies’ obligations to estimate, monitor, and report improper payments. It also directs agencies to report specifically on high-priority improper payments and make all reports available on a central website. It also speaks to the Do No Pay Initiative and facilitates computer matching of relevant information.
Generally speaking, the federal tactics to combat improper payments fall into a few categories: assessing the risk of fraud; estimating the impact of TPL; requiring more reporting, which in turn creates administrative burden; and efforts to increase data-sharing. By far the most efficient and effective of these tactics are those that increase data-sharing. When states improve timely access to accurate information on Medicaid beneficiaries, they greatly increase their chances at avoiding unnecessary costs and therefore decrease
the inefficient process of ‘pay and chase.’
As demonstrated in Figure 1, Medicaid improper payments more than tripled from FY 2014 to FY 2019, escalating from about $17 billion to now more than $57 billion. This suggests federal efforts to assess risk, estimate improper payments’ impact, and report related data are working. However, while more dollars are being reported, recoupment efforts are not yielding greater success. A few individual states
are making progress, but viewed nationally, improper payment rates are increasing at an alarming rate. Federal requirements like estimating and reporting can frame and detail this problem, but only more advanced data-sharing approaches can make a meaningful impact on this multi-billion dollar problem.
Cost Avoidance Makes More Sense Than Pay and Chase
Cost avoidance is more efficient than ‘pay and chase,’ plain and simple. If Medicaid plans can identify whether a plan member has primary coverage, before claims are paid, the need for post-payment recovery is mitigated. While improper payments may never be eliminated completely, employing a suite of technology solutions along the payment continuum can help Medicaid plans maximize the efficiency of their adjudication processes. In order to effectively engage in cost-avoidance, Medicaid programs need good quality data. They can discover third parties three ways:
- Self-reporting by beneficiaries, usually on Medicaid application forms
- State verification of beneficiaries’ self-reported data
- State matching of coverage files with those of other third-party payers
The subset of Medicaid members who have unreported primary commercial coverage present a tremendous opportunity for payers of last resort to “get in front” of the problem. With the timely delivery of accurate eligibility data on these members, improper claims payments and wasteful spending can be limited.
Unfortunately, discovery and verification often happen after enrollment. Medicaid may already be paying out claims when it finds other responsible third parties. The longer discovery and verification take, the greater the likelihood that there are claims accumulating in the ‘pay and chase’ queue. Technology offers part of the solution. By using electronic matching and reliable data, states can shorten the time discovery and verification take.
The Solution
Medicaid plans agree that cost avoidance makes more sense than ‘pay & chase’, but until now the ability to execute it effectively has not been widely available. Through Syrtis Solutions’ ProTPL program, accurate and active eligibility data can be delivered to payers of last resort in time to cost avoid claims and mitigate improper payments.
Syrtis Solutions is the only real-time source of primary commercial pharmacy and medical coverage data obtained through an ePrescribing master patient index (MPI). In order for an ePrescribing system to function, there must be an MPI that maintains consistent, accurate and current medical and eligibility data on the patients seen and managed within its various departments. Because the need for timely and accurate patient data necessitates the cooperation of health plans and PBMs to provide ongoing access to their member’s eligibility information, an ePrescribing MPI makes it a superior source of active and accurate eligibility information. Leveraging the largest MPI in the nation (280 million commercially covered lives) allows for more timely identification of TPL and allows for best-in-class OHI discovery.
Syrtis, with its vast experience in pharmacy operations and National Council for Prescription Drug Programs (NCPDP) standards, is the only vendor in the marketplace with the proprietary logic necessary to decipher the complex coding of pharmacy transactions and translate it into actionable eligibility data that can be utilized by payers of last resort to cost-avoid improper prescription and medical claims payments. Furthermore, Syrtis uses its superior matching algorithm to find primary coverage on members that no other vendor in the marketplace can find. Studies have demonstrated that up to 80% of the primary commercial coverage discovered via the ProTPL methodology cannot be found using any other existing process 23. Payers of last resort that utilize ProTPL achieve up to a 40% increase in discovery of primary payers (above and beyond any TPL processes). Most importantly, ProTPL is very easy to implement and once deployed, immediately mitigates improper claims payments and the need for ‘pay and chase.’
The U.S. government has expended a staggering quantity of resources trying to tackle the Medicaid TPL problem. It has passed laws, issued regulations, widened the net of entities that must cooperate, increased reporting standards, and enhanced data systems. Federal efforts to improve data sharing nationwide to tackle the TPL problem are important and ongoing. Right now, some of the best, most accurate data on patients’ health insurance coverage reside in ePrescribing infrastructures.
EPrescribing data certainly was not originally intended for these purposes. However, its potential to yield significant “low-hanging fruit” in the battle against ‘pay & chase’ is undeniable. ProTPL is not another recovery program. It addresses the problem of improper payments on the front end, gathering better data and applying them so as to avoid claims costs and the expenses associated with recovery efforts.
Those involved in the process of Medicaid claims payments have been operating with the best tools they had available. Now, they have a new and better tool through Syrtis Solutions’ ProTPL program.
How Do We Prospectively Identify TPL In Near Real-Time?
Through access and innovative use of nationwide e-prescribing networks.
The Largest Nationwide
E-Prescribing Network
Over 95% of the population’s Active Coverage information
All major commercial payers, PBMs, TPAs and self-funded employer groups participate
Eligibility Data is Active Coverage information and is 99.99% accurate
References
1 https://paymentaccuracy.gov/the-numbers/
2 https://www.govinfo.gov/app/details/CFR-2011-title42-vol4/CFR-2011-title42-vol4-part433-subpartD
3 https://www.everycrsreport.com/files/20101004_RL34164_05dafec1d2d13abb58d6337293029a83a4251d8b.pdf
4 https://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/Medicaid-and-CHIP- Compliance/PERM/index.html
5 https://www.congress.gov/bill/109th-congress/senate-bill/1932
6 Ibid.
7 https://www.gao.gov/assets/260/251526.pdf
8 https://oig.hhs.gov/oei/reports/oei-09-11-00780.pdf
9 https://obamawhitehouse.archives.gov/the-press-office/executive-order-reducing-improper-payments
10 https://www.congress.gov/bill/111th-congress/senate-bill/1508?q=%7B%22search%22%3A%5B%22s.1508%22%5D%7D&s=3&r=1
11 https://www.gao.gov/assets/670/668134.pdf
12 https://oig.hhs.gov/oei/reports/oei-05-11-00130.pdf
13 Ibid.
14 Ibid.
15 https://www.congress.gov/bill/114th-congress/senate-bill/2133q=%7B%22search%22%3A%5B%22Fraud+Reduction+and+Data+Analyt-ics+Act%22%5D%7D&s=5&r=1
16 https://fiscal.treasury.gov/DNP/
17 https://www.congress.gov/bill/114th-congress/house bill/2q=%7B%22search%22%3A%5B%22preventing+and+reducing+improper+medi-
care+and+medicaid+expenditures+act+of+2015%22%5D%7D&s=1&r=1
18 https://www.medicaid.gov/medicaid/data-and-systems/mmis/index.html
19 https://www.cms.gov/Research-Statistics-Data-and-Systems/Monitoring-Programs/recovery-audit-program-parts-c-and-d/Program-Histo-ry-and-Authorities
20 https://www.gao.gov/assets/690/688748.pdf
21 https://www.gao.gov/assets/690/688857.pdf
22 https://www.congress.gov/bill/116th-congress/senate-bill/375q=%7B%22search%22%3A%5B%22Payment+Integrity+Information+Act+of+2019%22%5D%7D&s=6&r=1
23 Case study conducted in 2016 with a state Medicaid agency.
24 Reviews with existing customers show 25% – 40% increases in OHI discovery rates once ProTPL was implemented.