 There are many reasons why improper payments occur in government-funded health care systems:
There are many reasons why improper payments occur in government-funded health care systems:
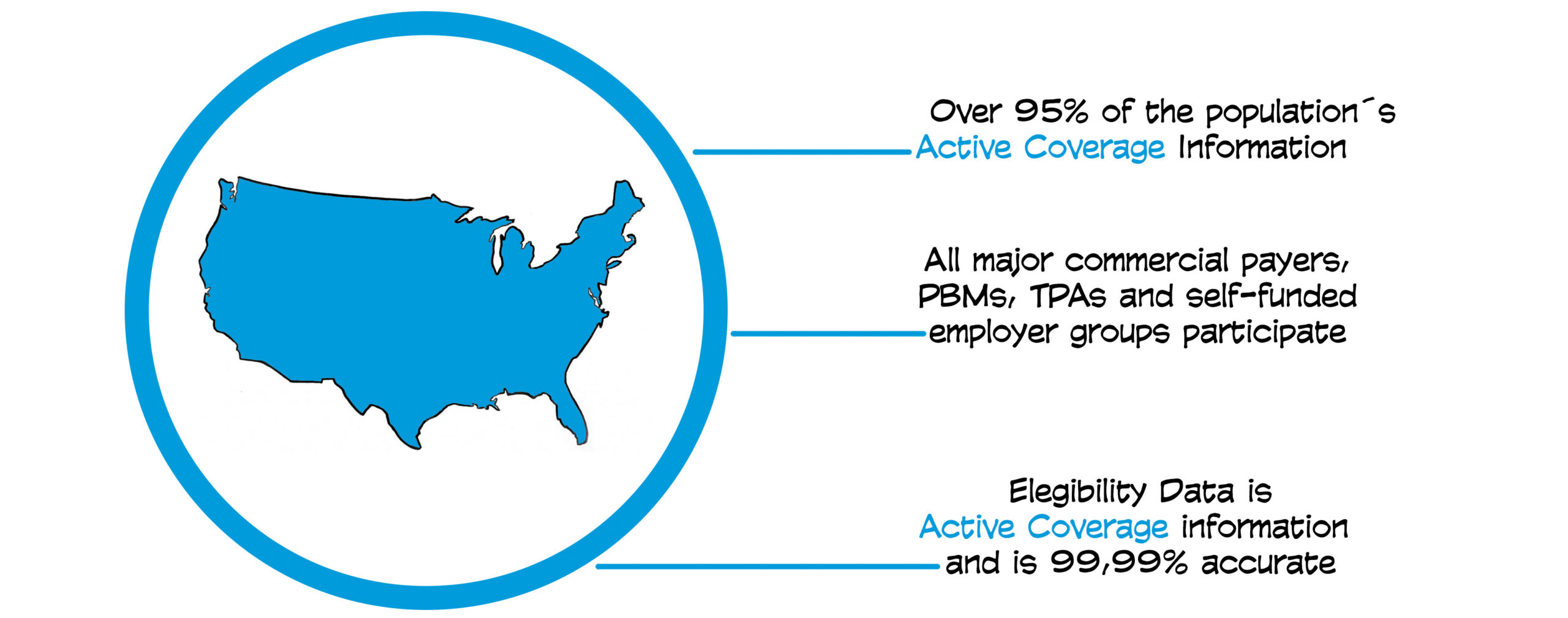
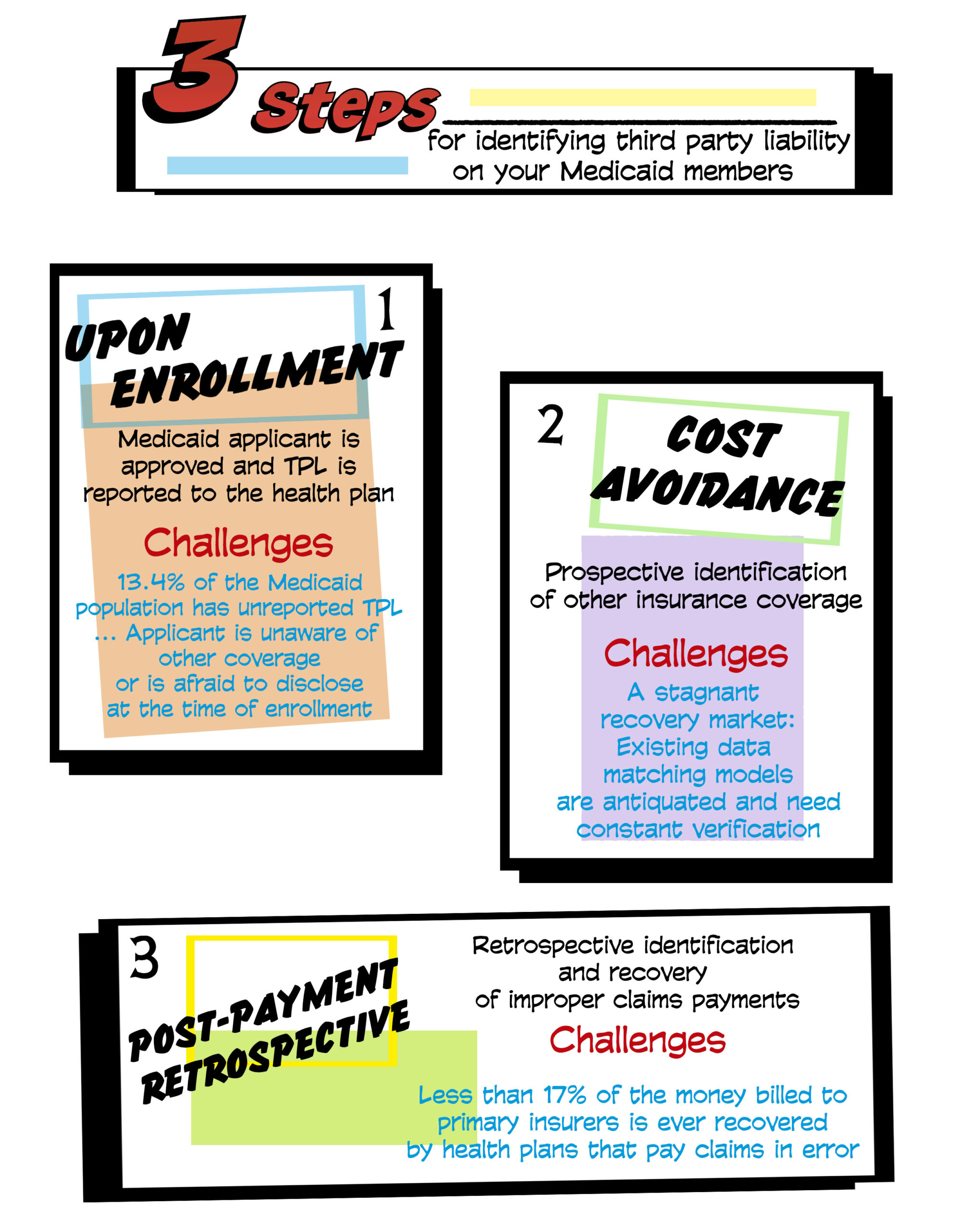
Coordinating benefits and determining third party liability (TPL) is complex, requiring timely data and the management of multiple data sources
The Medicaid population has a high rate of churn and is in near-constant flux
Eligibility data is not coordinated between federal and state systems and is often inaccurate
By law, Medicaid plans are payers of last resort. This means if a beneficiary has health care coverage through any other third party, that third party must pay its legal liability first. If any liability remains, Medicaid plans will then pay. According to the Centers for Medicare and Medicaid Services (CMS), “States are required to take all reasonable measures to ascertain the legal liability of third parties to pay for care and services that are available under the plan.”
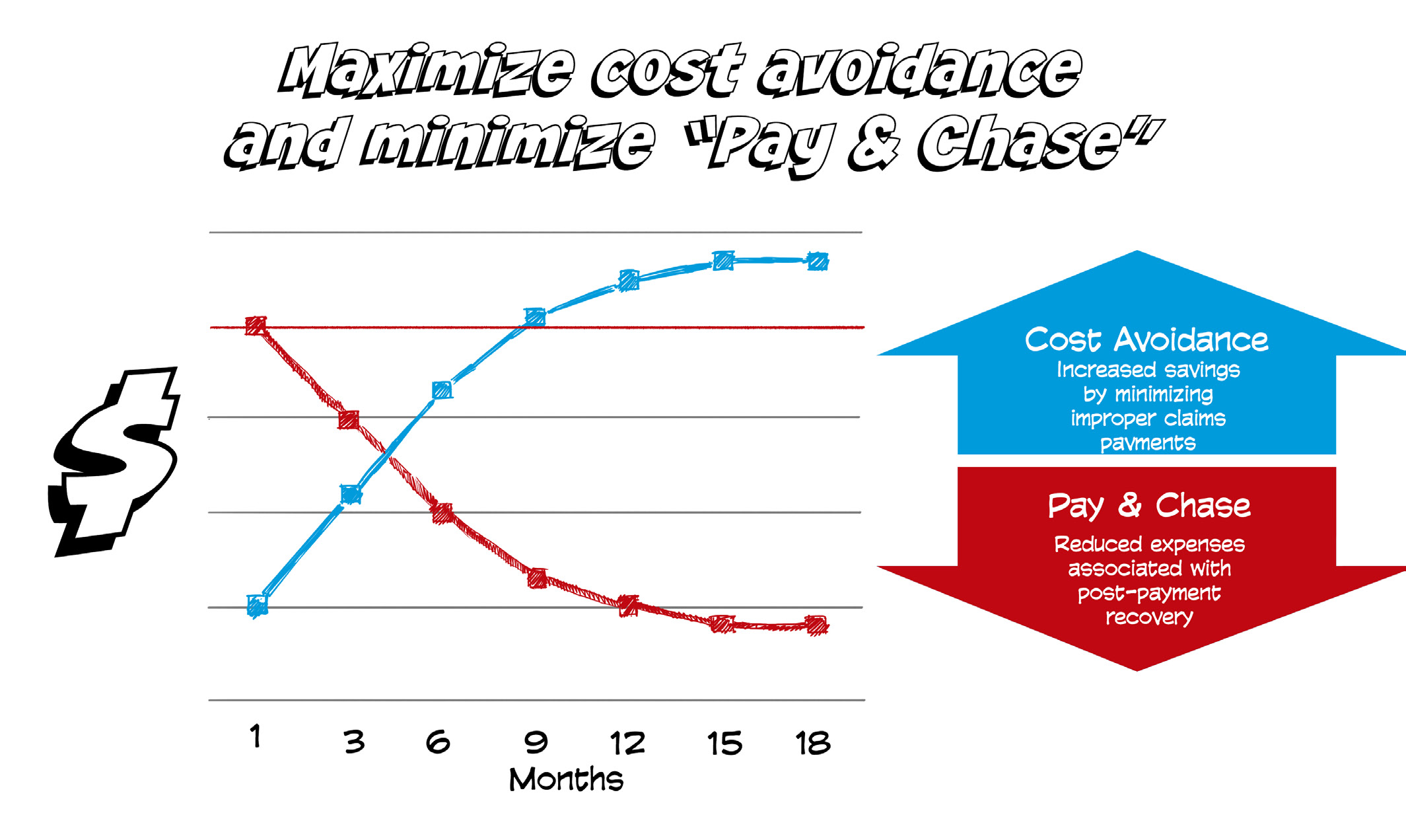
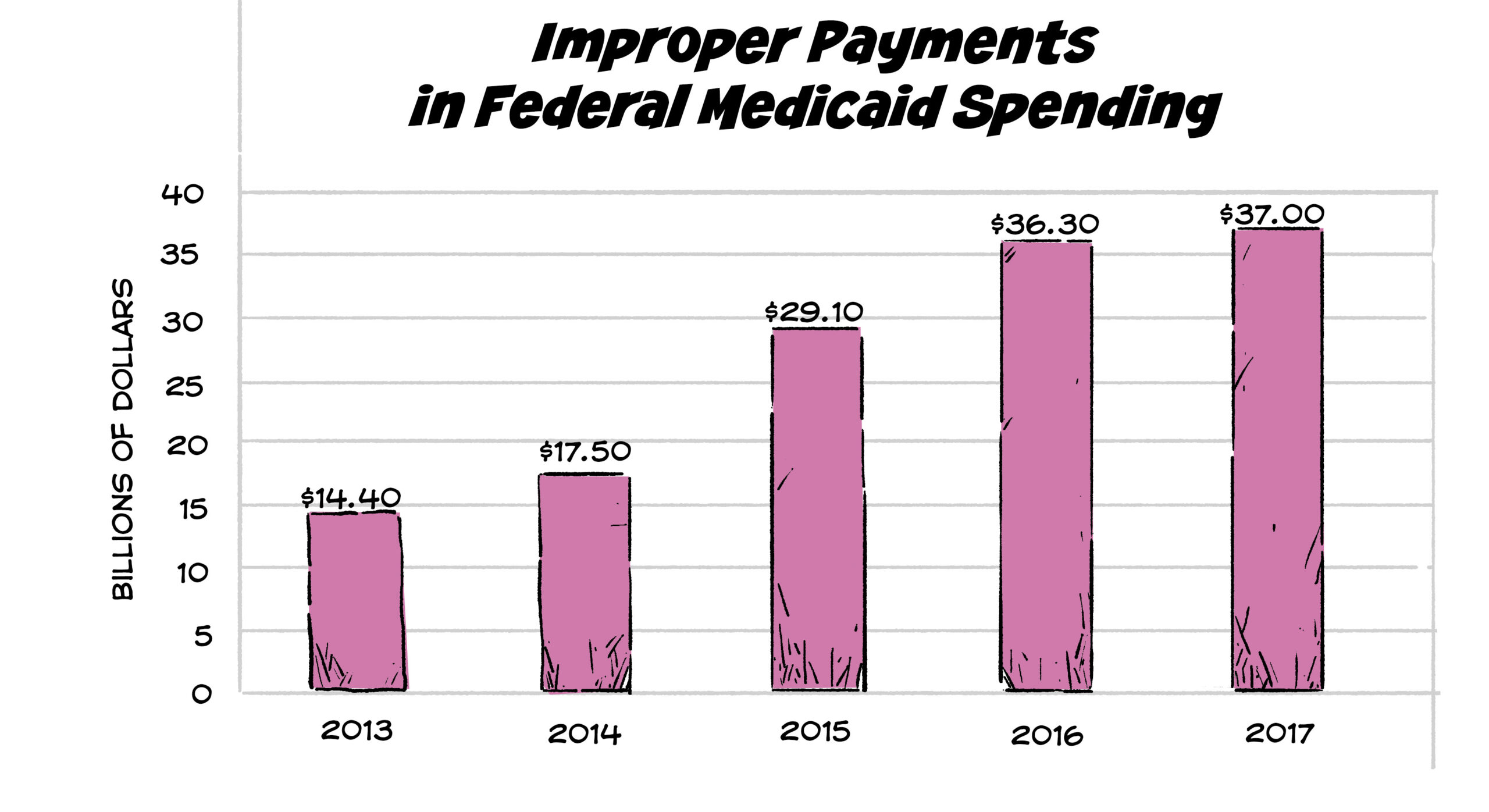
 Without reliable, complete, and accurate data, Medicaid plans often make claims payments in error, leading to one common course of action: “pay and chase.”
Without reliable, complete, and accurate data, Medicaid plans often make claims payments in error, leading to one common course of action: “pay and chase.”
The ability to identify liable third party payers before claims are improperly paid has been a chronic challenge due to:
Antiquated technology
Siloed data systems
Network latency
“Pay and chase” occurs when:
Payments are made in good faith by a payer of last resort.
That payer later discovers the payments were made in error and were actually the responsibility of another third party payer.
The payer of last resort then attempts to recoup the funds from the responsible third party payer.
Because of unreliable eligibility data, Medicaid plans frequently pay claims that are not, in fact, their responsibility. When new eligibility information or updated data becomes available and plans uncover overpayments, the “chase” begins.
Federal payer of last resort programs such as Medicaid have been allowed to pay claims in error and pursue reimbursements for two primary reasons. First, CMS has widely approved waivers to the cost avoidance directive. Second, there is an obvious need to recover claims payments when third party liability (TPL) is identified retrospectively.
The practice of ‘pay and chase’ has become normalized, even though cost avoidance and routing claims to the proper payers is the only way to ensure federal dollars are not paid in error. Furthermore, an entire multi-billion-dollar industry has been built around post-payment recovery. Unfortunately for payers trying to recoup improper claims payments, the actual funds recovered remain around twenty cents on the dollar.
On another, practical front, it is understandable that plans may sometimes pay so as not to drag out the claims payment process. When coordinating benefits causes claims payments to be delayed, providers become dissatisfied, and this could result
in providers choosing not to participate in Medicaid.5 There is already a shortage of providers willing to accept Medicaid, so rather than exacerbate this problem; Medicaid plans pay, even if it means they will have to chase those dollars later.